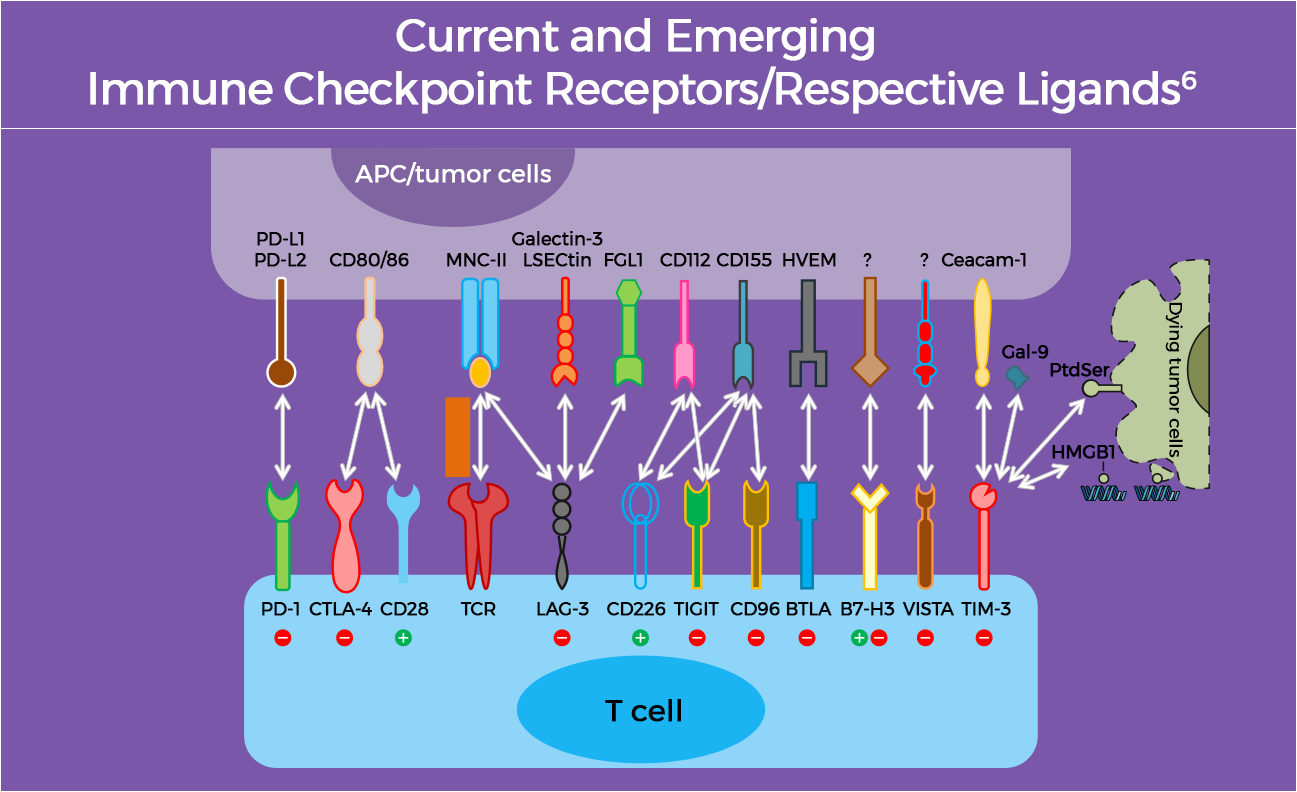
Another checkpoint protein, PD-1, plays a major role in regulating immune responses in peripheral tissues. Binding of PD-1 to its ligands PD-L1 and PD-L2 suppresses T-cell activation and function, leading to a diminished immune response against tumor cells.6 Therapies that target PD-1 or PD-L1 inhibit this binding and restore antitumor immune response.4 Several PD-1 inhibitors are currently FDA-approved for treatment of various malignancies, alone or in combination with other agents and across many disease settings. These include the PD-1 inhibitors pembrolizumab, nivolumab, cemiplimab, dostarlimab-gxly, penpulimab-kcqx, retifanlimab-dlwr, and tislelizumab-jsgr, and the PD-L1 inhibitors atezolizumab, avelumab, and durvalumab.4,5